Promoting health and striving to reduce inequities
Socio-economic disparity affects the prevalence of non-communicable diseases. Populations of lower socio-economic status are more likely to develop non-communicable diseases and suffer greater exposure to related risk factors, while rates of obesity are also higher and are increasing more rapidly among these groups.
In response, in 2012 the EPHE (EPODE for the Promotion of Health Equity) project was launched, aiming to reduce socio-economic inequities linked to health-related behavior of families in 7 European countries over three years.
Discover the whole story EPHE from theory to practice!
Why EPHE?
The prevalence of overweight and obesity in childhood has increased remarkably in developed countries, from 17% in 1980 to 24% in 2013 in boys and from 16% to 23% in girls. Similarly, in developing countries, rates have risen from roughly 8% to 13% in both boys and girls over the three decades.
2.1 billion people — nearly 30% of the world’s population — are either obese or overweight.
40% of overweight children will continue to have increased weight during adolescence and 75−80% of obese adolescents will become obese adults.
2.1 billion people — nearly 30% of the world’s population — are either obese or overweight.
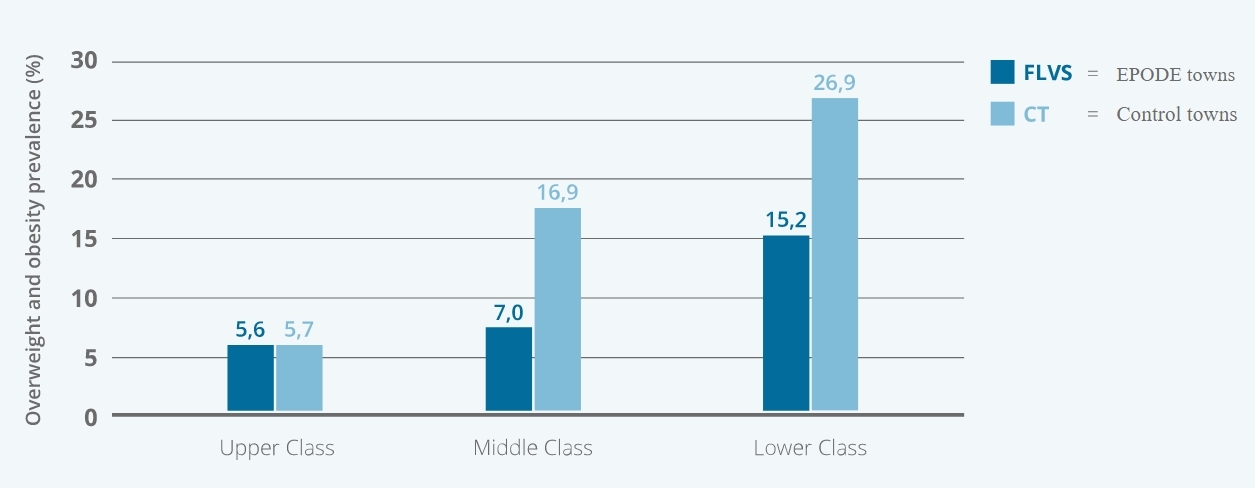
Adults in lower income categories are experiencing higher levels of obesity than adults in high income groups. The social gradient can account for around 25% of the obesity prevalence in men and 50% in women.
Not only is the obesity crisis weighing heavy on public health, it is also a burden to public funds, with obesity representing an estimated 1% to 3% of total health expenditure in most countries.
Obesity is preventable in all populations. That’s what the EPODE pilot study demonstrated from 1992 to 2004 in the North of France by taking a series of coordinated societal measures, slowing down the obesity trend and enhancing a healthy active lifestyle among children.
EPODE enables communities to implement effective and sustainable strategies to prevent childhood obesity. Its philosophy includes a positive, step-by-step approach, without any stigmatisation, tailored to the needs of all socio-economic groups.
The EPHE project seeks to reduce the health gap
between socioeconomic groups in 4 main areas:
Drink enough clean water a day. At least two liters.
Eat fresh fruits and vegetables. Replace snacks with healthier snacks.
Maintain an active lifestyle. Walk at least 10,000 steps a day.
Get some sleep. Get at least eight hours of sleep a night.
Participating in this Project are…
EPHE brings together many different actors in order to achieve our objectives. Click on the icons below to learn more about the roles of each participating actor.
Community-Based Programmes
A Community-Based Programme is an organized programme within the community which carries out « interventions » or actions in its schools and family settings with the community at large. Political endorsement and multi-stakeholder support is crucial.
Experts
The EPHE Scientific Advisory Board is composed of representatives from European universities, experts in the fields of physical activity and nutrition.
European Union
The European Union is a funding partner of the EPHE project. The endorsement of this body is significant as it underlines the credibility of the project and facilitates its outcomes dissemination across Europe.
Private Partners
Public-Private Partnerships is one of the pillars of the EPODE Methodology at local and central level. Discover more about the EPHE co-funding partners and their rules of engagement.
The EPHE project works with 7 European cities from
7 Community-Based Programmes to conduct its pilot-life study.
Maia Menu Saudável
Portugal, Maia
Since 2006
School-based programme in the Municipality of the city Maia, promoting healthy eating habits and lifestyle to over 8.000 school children
EPODE
France, Flandre-Lys
Since 2003
8 cities extending to 38.932 inhabitants
Viasano
Belgium, Mouscron
Since 2007
20 cities, activating 815.000 inhabitants
JOGG
Netherlands, Zwolle
Since 2010
More than 75 cities, reaching over 1 million people (including + 300.000 children!) and enabling them to make healthy lifestyle choices
I’m living healthy, too! – SETS
Romania, Otopeni
Since March 2011
252 schools in Bucharest, involving over 94.500 students, along with their families
Paideiatrofi
Greece, Maroussi
Since 2008
9 PAIDEIATROFI towns, reaching out to 30.000 children and their families
Healthy Kids in Bulgaria
Bulgaria, Triaditsa, Studenski and Lyulin
Since 2011
3 regions in the Capital Sofia, stimulating over 5.000 primary school children
Guidance from an experts' committee
Click on the logo of each of our scientific partners to learn more about their involvement.
Evaluations & Results
In order to measure the evolution in terms of behavior change as a result of the EPHE interventions, 3 key stages to the evaluation process were devised.
Baseline evaluation by the scientific partners to understand behaviors before the EPHE interventions began
Evaluation to identify if and how the EPHE interventions have a positive impact on behaviors
Evaluation to determine whether the interventions have a sustainable impact on energy-balance related behaviors
Conclusions
Public & Private Partners Collaborating for Health
This web platform is the result of the European project, “EPODE for the Promotion of Health Equity” (EPHE, agreement number: 2007327). This project has received funding from the European Union, in the framework of the Health Programme.
The EPHE project is also co-funded by private partners that have committed to the EU platform on diet, physical activity and health and signed a commitment charter for the project.